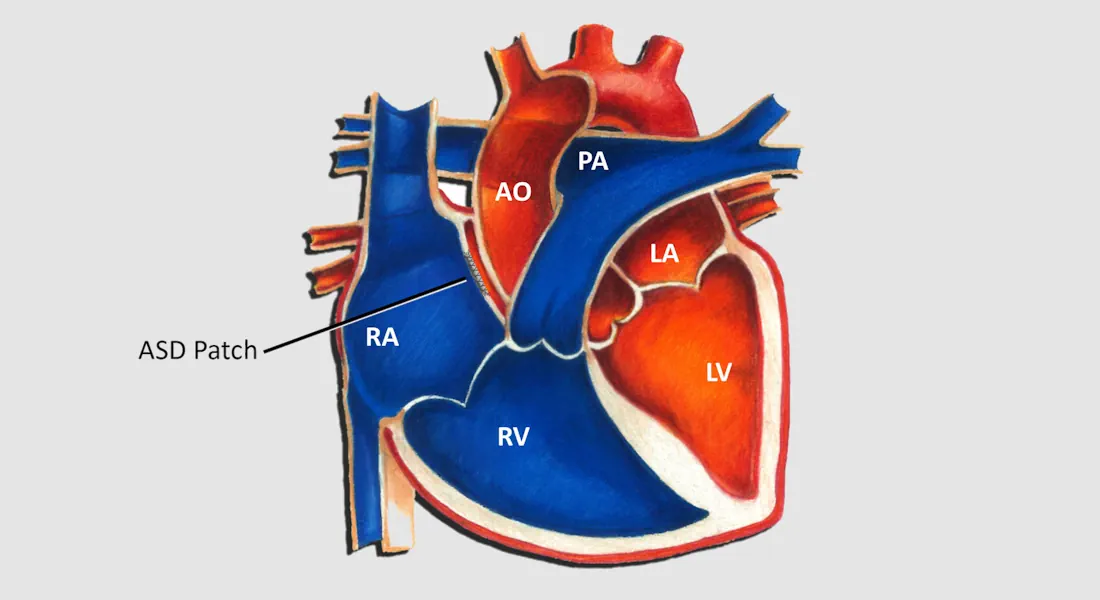
Some people are born with congenital heart defects, such as an atrial septal defect (ASD). This condition involves a hole between the heart’s two atria, which can cause shifts in heart pressure and potentially lead to strokes. When indicated, individuals, often young, may seek keyhole closure of this defect. This minimally invasive procedure, in experienced hands, offers rapid relief and a quick return to normal activities.
Please send us your message and we will contact you as soon as possible